




























Healthcare has no shortage of impressive AI demos. The harder question is why so few of them make it into the daily rhythm of care. In 2026, the bottleneck is rarely the model. It is the gap between what AI can do and how work is actually done, the handoffs, the exceptions, the legacy systems, and the people who have to trust the output. This article looks at why workflow, not technology, is where healthcare AI succeeds or stalls, and what organizations that are getting it right do differently. When AI is embedded into real clinical workflows, the result is not just operational efficiency, but earlier diagnoses, fewer missed follow-ups, and more consistent, equitable patient care. Poorly designed workflows, by contrast, turn even the best models into unused tools.
The Gap Between Capability and Operations
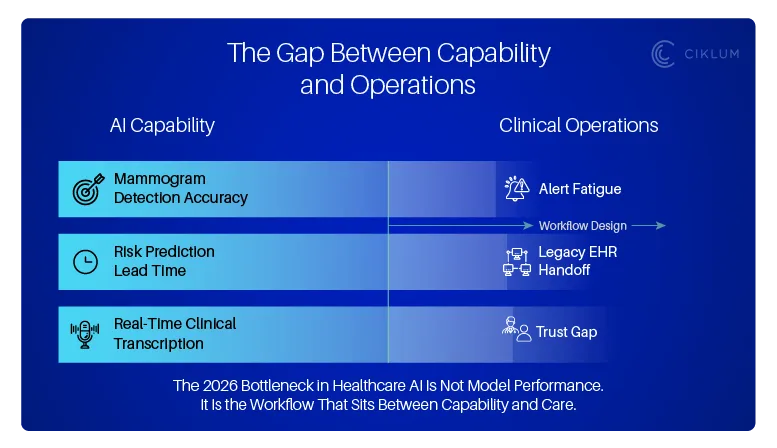
Healthcare AI has crossed a threshold. Models can now detect breast cancer in mammograms with accuracy that matches or exceeds radiologists. Predictive tools identify high-risk patients before symptoms appear. Natural language systems transcribe clinical notes in real time. The capability is no longer in question.
What is in question is whether healthcare organizations can embed these capabilities into the way work actually happens.
The State of Clinical AI Report 2026 makes this plain: while AI models show major leaps in actionable prediction and autonomous reasoning, human-computer workflow design remains the critical weak point. There is significant room for improvement in how AI fits into clinical processes, how failure modes are handled, and how automation bias is mitigated.
A primary symptom of this gap is "Alert Fatigue." When AI is layered onto a workflow without design discipline, it often manifests as a barrage of notifications that clinicians eventually learn to ignore. Even a highly accurate model becomes a liability if its insights are buried under a mountain of digital noise. In a high-stakes clinical environment, "more data" is rarely the answer - the goal must be "better-timed intelligence."
In other words, the technology is ready. The workflows are not.
The Staffing Crisis Makes This Urgent
This is not an abstract design challenge. The healthcare workforce is under sustained pressure that is not going to reverse on its own.
The World Health Organization projects a global shortfall of 11 million health workers by 2030. In the US, the American Hospital Association's 2026 Workforce Scan identifies the need to fundamentally redesign staffing models, upskill existing teams for digital fluency, and improve engagement and well-being as top priorities.
Meanwhile, 1 in 4 healthcare providers are considering leaving the profession due to burnout and 82% of healthcare insiders believe AI-assisted workflows can help. That belief is well-founded, but only if AI is applied to the right problems in the right way.
The opportunity is not to replace clinicians. It is to remove the administrative friction that pulls them away from patient care (the scheduling, the documentation, the claims processing, the compliance reporting) so they can focus on the work that requires human judgment. In practice, this translates into shorter wait times, more time per patient, faster care decisions, and reduced risk of errors caused by overload and fragmented handoffs.
Where Workflow Redesign Actually Delivers
The pattern emerging across organizations that are making progress with healthcare AI is consistent: they start with the workflow, not the model.
Claims and Revenue Cycle
AI and automation are now the leading revenue cycle investment priorities for health systems in 2026. The reason is straightforward: claims processing is high-volume, rule-heavy, and error-prone. Automating document extraction, eligibility verification, and denial management does not require frontier AI. It requires well-designed automation layered into existing workflows with clear handoffs, exception routing, and quality checks built in.
Organizations that approach this as a workflow redesign problem, rather than a technology deployment problem, consistently report faster processing, fewer errors, and measurable ROI. Google has found that nearly three-quarters of organizations using AI in healthcare are already generating positive return on investment, and some hospitals report saving $3.20 for every dollar invested.
Audit and Compliance
Regulatory reporting is another area where the work is well-defined but the execution is manual and fragile. A billion-dollar pharmaceutical company addressed this by building an ML pipeline that analyzed over 400,000 audit findings, replacing error-prone manual categorization with automated, explainable tagging. The model did not just speed up the process, it gave leadership confidence in the results, because every categorization could be traced back to the underlying data.
The lesson: compliance AI works best when explainability is designed in from the start, not bolted on after deployment.
Clinical Administration
The administrative burden on clinicians is enormous. Documentation, scheduling, prescription renewals, intake forms, these tasks are individually small but collectively account for hours of a clinician's day. A regenerative medicine nonprofit cut two hours of latency per opportunity for its field teams by automating document creation and standardizing workflows across the enterprise using Salesforce Sales Cloud.
The same principle applies to clinical settings. When agentic AI systems handle the transcription, the routing, and the follow-up scheduling, clinicians get time back and patients get more of their attention.
What the Winners Do Differently
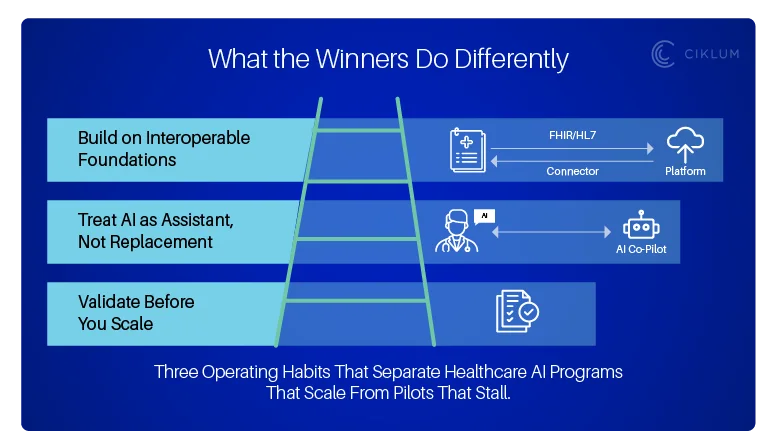
The organizations generating value from healthcare AI share three habits:
1.They validate before they scale. The most common failure pattern in healthcare AI is building a pilot that works in isolation but stalls when it meets real clinical workflows, legacy systems, and change-resistant teams. Successful organizations invest in problem validation first confirming the problem is real, the data is viable, and the workflow is ready before writing a line of code.
2.Successful organizations treat AI as an assistant, not a replacement. They delegate routine tasks to models while reserving high-stakes oversight for clinicians. This "Human-in-the-Loop" approach relies on User Personas to ensure tools respect the unique cognitive loads of different medical roles. By co-designing alongside nurses and doctors, developers can identify and remove the friction that often leads to "breaking points" in care. Ultimately, AI built with clinicians feels like a natural extension of the team rather than an administrative intrusion.
3.AI cannot operate reliably on fragile or "siloed" infrastructure. The organizations making progress have moved beyond legacy bottlenecks by investing in API-first architectures and HIPAA-compliant cloud platforms. Crucially, they prioritize interoperability by adopting FHIR (Fast Healthcare Interoperability Resources) standards. This ensures that the AI model isn't just a "black box" sitting on a server, but a functional part of the ecosystem that can pull and push data seamlessly across Electronic Health Records (EHRs). By combining these modern data standards with infrastructure-as-code and automated CI/CD, they ensure that when AI is introduced, it has a stable, secure, and scalable foundation to run on.
The Question for 2026
Healthcare AI is no longer about whether the models work. It is about whether organizations can redesign the workflows, the infrastructure, and the governance to let them work in practice.
The staffing crisis is not going to wait. Neither will the patients who depend on systems that are already stretched thin. The question is not whether to invest in AI, it is whether to invest the discipline to get the workflow right first.
That discipline is what separates a pilot from a program, and a program from a system that actually improves care.
Ciklum works with healthcare organizations to design and build AI-powered workflow automation with the governance, infrastructure, and human-in-the-loop design to operate at scale.
If you are planning your next step, we would welcome the conversation.
By Ciklum Editorial Team

Ciklum’s Editorial Board is a collective of experienced writers and industry experts, bringing together perspectives shaped by real-world engineering and delivery experience. Through collaborative insights, the team explores how technology, AI, and digital innovation move from concept to execution across industries.
Blogs
Discover Similar Insights

Building Trustworthy and Scalable AI Models for US FinTech Compliance
Learn More
From Diagnosis to Claims: Where AI Actually Works in Healthcare
Learn More
Cloud Engineering for HIPAA: Secure Configuration and Migration Strategies for US Healthcare Providers
Learn More
Agentic AI and the Future of Personalized Healthcare
Learn More